# Seborrheic Keratoses (지루각화증)
---
## 1. Definition
- **Seborrheic Keratoses (지루각화증)** are **benign epidermal tumors** arising from keratinocytes.
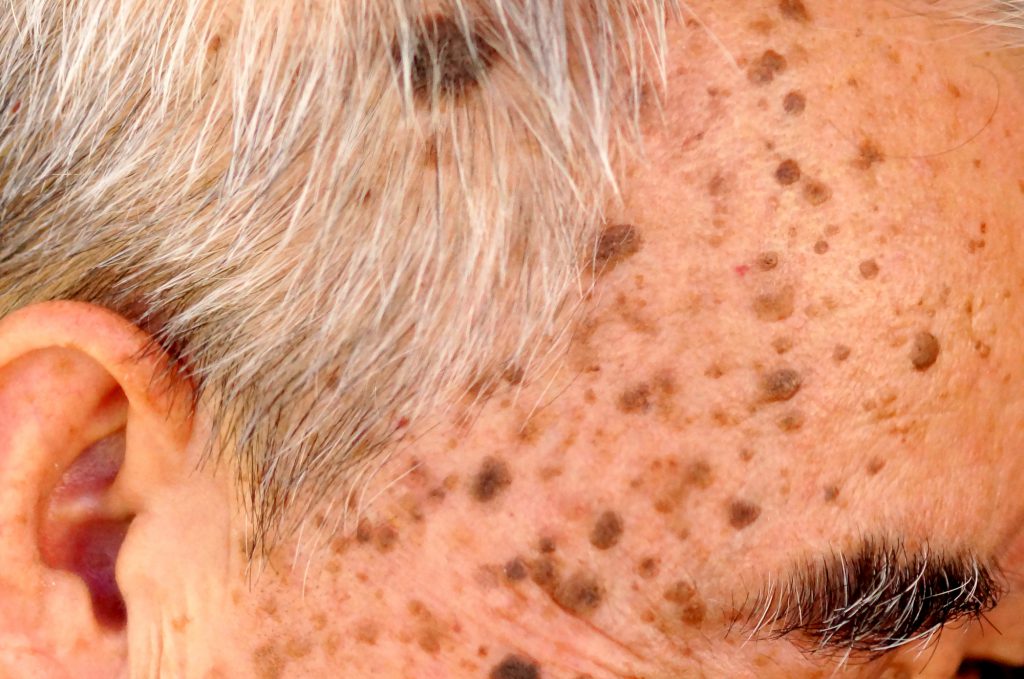
- Clinically: pigmented, verrucous, “stuck-on” plaques.
- Pathologically: acanthosis, hyperkeratosis, and horn cysts without cytologic atypia.
---
## 2. Epidemiology & Prevalence
- **Most common benign epithelial tumor in adults.**
- **Prevalence**:
- By age 40 → ~30% of population.
- By age 60 → >80% have at least one lesion.
- Nearly **universal in elderly**.
- No gender predilection.
- More common in **lighter phototypes (I–III)**, but dermatosis papulosa nigra variant is frequent in darker skin (particularly in African and Asian populations).
- Rare in children and young adults → onset typically after 30s.
---
## 3. Pathophysiology
### A. Cellular Basis
- Originates from **epidermal keratinocytes**.
- Characterized by:
- **Hyperproliferation** of basal keratinocytes.
- **Accumulation of keratin** → hyperkeratosis and horn cysts.
- **Basaloid cell nests** → proliferation without atypia.
### B. Molecular Mechanisms
- **Genetic mutations** implicated:
- **FGFR3** (fibroblast growth factor receptor 3) mutations.
- **PIK3CA** mutations (PI3K-AKT pathway activation).
- Lead to **increased keratinocyte proliferation** but no malignant transformation.
- **UV radiation**: associated with solar-exposed SKs (solar lentigo-like).
- **Aging process**: cumulative epidermal damage + senescent keratinocyte dysregulation.
- **HPV**: controversial, but some evidence of low-risk HPV DNA in lesions.
### C. Systemic Association
- **Leser-Trélat sign (레저-트렐라 증후군)**: sudden eruption of multiple seborrheic keratoses associated with internal malignancy (esp. GI adenocarcinoma).
- Rare but clinically important → warrants systemic work-up if rapidly progressive SKs appear with systemic symptoms.
---
## 4. Clinical Presentation
- **Morphology**: sharply demarcated, waxy, “stuck-on,” verrucous plaques.
- **Colors**: light tan → dark brown → black.
- **Variants**:
- Dermatosis papulosa nigra (흑인·동양인에서 작은 다발성)
- Stucco keratoses (작고 흰색, 각질성, 주로 하지)
- Irritated seborrheic keratosis (홍반, 가려움, 딱지 동반)
---
## 5. Histopathology
- **Acanthosis**: thickened epidermis.
- **Hyperkeratosis**: excess keratin at surface.
- **Horn cysts**: round keratin-filled cysts → pathognomonic.
- **Basaloid cell proliferation** without atypia or dermal invasion.
---
## 6. Differential Diagnosis
- **Melanoma (흑색종)** – irregular borders, color variegation, bleeding.
- **Pigmented basal cell carcinoma (기저세포암)** – pearly papule with telangiectasia.
- **Actinic keratosis (광선각화증)** – premalignant, scaly erythematous plaques.
- **Solar lentigo (노인성 색소반)** – flat brown macules, no verrucous surface.
---
## 7. Treatment
- Only if: cosmetic concern, irritation, or diagnostic uncertainty.
- **Options**:
- Cryotherapy (냉동치료) → thin lesions.
- Curettage (소파술) → scraping off.
- Electrocautery (고주파 소작술).
- **CO₂ Laser (이산화탄소 레이저)** → gold standard for raised SK, precise ablation.
---
## 8. Prognosis & Patient Education
- Benign, no malignant potential (except in Leser-Trélat sign context).
- Lesions may recur or new ones appear with aging.
- Patients should be reassured but educated about the **“ugly duckling sign”**—any lesion that looks different should be biopsied.
---
✅ **Key Pearls for Practice**
- **Extremely common** in elderly, almost universal.
- **Pathophysiology**: keratinocyte proliferation driven by **FGFR3 / PIK3CA mutations**.
- **CO₂ laser** is the treatment of choice for cosmetic removal.
- Watch for **Leser-Trélat sign** → possible paraneoplastic syndrome.
---